
Tooth Movement: The Third Rail of Sleep Apnea Appliances
CAD-CAM Sleep Apnea appliances such as the Narval CC by ResMed and D-SAD by Panthera incorporate a unique band of nylon that attaches the right and left side without contacting the anterior teeth. The design of this band is in our control when prescribing these devices and selecting the wrong design can result in unfavorable outcomes, potentially impacting on ”Tooth Movement” and ”Retention”.
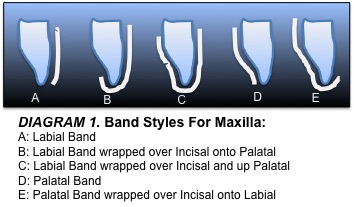
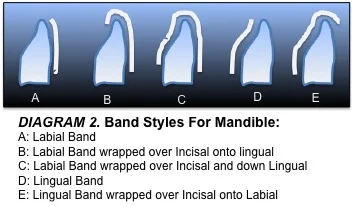
In Diagram 1 and 2 below a mid-sagittal cross section view shows the device and dentition depicting the various band designs. These bands can run along the Labial exclusively, Lingual/Palatal exclusively, or they can run over the Incisal edge incorporating both the Labial and Lingual/Palatal.
First, let’s talk about the impact these bands have on tooth movement. As we all know, teeth move when forces are placed on them. Since wearing a Sleep Apnea oral appliance results in some level of pressure on the teeth, one can safely assume that these appliances are likely to cause tooth movement. What we are learning is that this tooth movement varies depending on appliance design and that sometimes we do have a certain level of control over that design. This is the case with the bands used in CAD-CAM Sleep Apnea oral appliances. When one designs the band to run over the Labial of the maxillary anteriors (which is the default design for both the Narval and D-SAD), the tongue which moves forward along with mandibular advancement places a gentle pressure up against the Palatal of the maxillary anterior dentition. This pressure, given sufficient time, is likely to cause the maxillary anterior teeth to move Labially, creating interproximal spacing. The first patient I noticed this tooth movement on was myself. Interestingly, when I wore my Herbst appliance for a week, the diastema that had appeared between my centrals while wearing the Narval closed up completely. When I returned to wearing the Narval, the diastema reappeared.
Initially, I simply accepted my new diastema, and it took the following patient situation for me to take this seriously regarding the patients I treat. The wife of a long-standing patient came to see me for an appliance. Her husband, who first wore a Silencer and then transitioned to a Somnodent over a 12-year period, wanted her to get a Somnodent as he was having such a good experience with it. Upon seeing the Narval, she chose it over the other offerings due to its small size. All went well regarding the management of her snoring and mild OSA, however, within just a few weeks of wear, she developed a diastema between her two maxillary centrals that was far from small and increasing with passage of time. I requested that a new appliance be made due to the patient’s “complaint/side effect” and was able to have the appliance remade with a Palatal band with Incisal wrap (Diagram 1-E). It took a while, perhaps 2-3 months, but the diastema closed completely while continuing to wear her new Narval with the Palatal band design. Closure of the diastema required no further effort on my part aside from selecting the correct band design for this particular patient.
When selecting which band design to use on the maxilla I like to consider the starting point. Are the maxillary anteriors already in an ideal bite that the patient would prefer to protect? Are diastemas already present? Is there crowding that could benefit from some Labial repositioning? Are the teeth biting in an end-to-end relationship, which could also benefit from some anterior repositioning? Etc. When the objective is to absolutely minimize tooth movement I tend to prescribe the Palatal band with Incisal wrap (Diagram 1-E). There have been reports that some but not all patients develop the habit of rubbing up against the lower edge of the band if the palatal band design is used (Diagram 1-D), so wrapping the band around the Incisal onto the labial provides a smooth surface for the tongue to rub up against. So, it’s a good idea to treatment plan around this issue before prescribing these appliances. In some cases, the tooth movement associated with the Labial band may be desirable; it’s nice to have some level of control over this in our treatment planning, and it’s better to manage this issue prior to ordering the appliance in the first place. Whatever the situation, full disclosure to the patient regarding any tooth movement you anticipate occurring is a must.
Now, let’s talk about how these bands impact on retention. Initially, the Narval had these bands run across the Labial of the dentition solely, and the D-SAD had them run across the Labial for the maxilla and the Lingual for the mandible. However, in cases of shorter mandibular teeth lacking in undercuts for retention it was discovered that wrapping the mandibular band over the Incisal edge and down the other side made the mandibular portion of the appliance much stiffer. This allowed the retentive undercuts to be paired up from one quadrant to the other rather than depending solely on pairing them from within the same quadrant. The ability to engage undercuts from both sides of the arch substantially decreased the number of appliances being rejected for lack of retention. So, in cases where you are questioning adequacy of retention I recommend using a full coverage band, or coverage that runs over the Incisal edge to the other side. Since at the design stage the manufacturer has all the required information, I typically authorize them to make the best decision on this issue, full or partial wrap.

It turns out that aside from simply holding the two sides of the appliance together, these bands play a significant role in appliance retention and also minimizing or perhaps even eliminating certain tooth movement, ultimately impacting on outcome. In case you’re wondering, I am still walking around with a diastema!